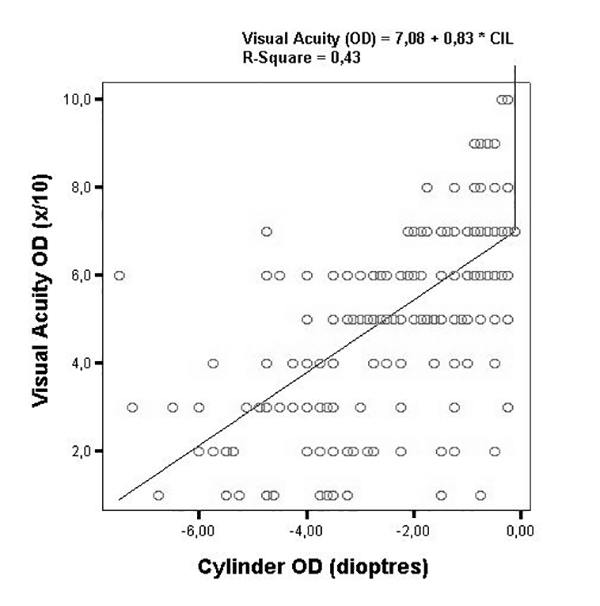
Figure 1. Correlation between visual acuity and astigmatism of the right eyes.
Prevalence of high astigmatism in Salta province, Argentina
Luis Zemana, Ruben D. Danzab, Laura Fejermanc, Rafael Iribarrend
a Departamento de Oftalmología, Hospital de Clínicas, Universidad de Buenos Aires, Buenos Aires, Argentina.
b Segunda Cátedra de Oftalmología, Hospital de Agudos Carlos G. Durand, Universidad de Buenos Aires, Buenos Aires, Argentina
c Department of Public Health, School of Medicine, University of California Davis, Davis, California.
dDrs. Iribarren Eye Consultants, Buenos Aires, Argentina.
Received: June 4th, 2021.
Accepted: July 28th, 2021.
Dr. Luis Zeman
luiszemanbardeci@gmail.com
Oftalmol Clin Exp (ISSN 1851-2658)
2021; 14(3): 162-170.
This submission has not been published anywhere previously and it is not simultaneously being considered for any other publication.
Conflict of interest: None of the authors have any proprietary interests or conflicts of interest related to this submission.
Financial Support: None.
Aknowledgments
Authors want to thank Prof. Mehdi Khabazkhoob and Prof. Akbar Fotouhi (Iran) for their help with the tables of refractive error in different countries, Prof. Andrea Molinari (Ecuador) for his help providing the data of Ecuatorian children, and Prof. Jason Yam (Hong Kong) for his help with the data from Hong Kong, and Prof. Siofra Christine Harrington (Ireland) for her help with the data from Irish children.
ABSTRACT
Purpose: Refractive errors are the first cause of visual impairment across the world. Prevalence data are crucial for planning visual health strategies, since early detection and treatment of refractive errors in children has a key role on normal vision development. This is the largest report in Argentina that has studied refractive errors under cycloplegic refraction in school-aged children.
Methods: Cross-sectional population based study, which involved school children aged 4-15 year-old examined from March to November 2014. Automated cycloplegic refractive error measurement and subjective refraction were performed. Myopia was considered as the spherical equivalent refractive error <-0.50 diopters, hyperopia as > +2.00 D. For the purpose of this study, astigmatism was considered as that equal or greater than -2.00 diopters.
Results: The sample consisted of 1852 children aged 8.03 ± 2.57 years, range 4 to 15 years of whom 967 (52.2%) were females. 116 subjects (6.26%) had a spherical equivalent lower or equal than -0.50 diopters and there were 111 (5.99%) subjects with refractive cylinder ≤ -2.00 diopters (limit -7.50 diopters). In the Seclantas zone (mountainside) the sample comprised 157 children, of whom 20 (12.75%) had astigmatic values in the right eyes ≤ than -2.00 diopters.
Conclusion: An elevated prevalence of high astigmatism and a very low prevalence of myopia were found in this population. Future studies including diverse populations with high prevalence of high astigmatism could contribute to a better understanding of the relevant factors in the etiology of this trait.
Keywords: myopia, astigmatism, school children, epidemiology.
Prevalencia de astigmatismo alto en la provincia de Salta, Argentina
RESUMEN
Objetivo: Los defectos refractivos son la primera causa de discapacidad visual. Los datos de prevalencia son cruciales para la planificación de estrategias de salud visual, ya que la detección y el tratamiento precoz de los errores de refracción en niños tienen un papel fundamental en el desarrollo normal de la visión.
Métodos: Estudio transversal poblacional en el que participaron escolares de 4 a 15 años examinados desde marzo a noviembre de 2014. Se realizó la autorrefractometría bajo cicloplejía y la refracción subjetiva. Se consideró la miopía como el error de refracción para un equivalente esférico <-0,50 dioptrías, y la hipermetropía como aquel >+2,00 D. A efectos de este estudio, se consideró el astigmatismo igual o superior a -2,00 dioptrías.
Resultados: La muestra estaba formada por 1.852 niños de 8,03 ± 2,57 años, con un rango de 4 a 15 años, de los cuales 967 (52,2%) eran mujeres. De ellos, 116 sujetos (6,26%) tenían un equivalente esférico inferior o igual a -0,50 dioptrías y había 111 (5,99%) sujetos con cilindro refractivo ≤ -2,00 dioptrías (límite -7,50 dioptrías). En la zona de Seclantas (alta montaña) la muestra comprendía 157 niños, de los cuales 20 (12,75%) tenían valores astigmáticos en los ojos derechos ≤ a -2,00 dioptrías.
Conclusiones: Se encontró una elevada prevalencia de astigmatismo alto y una muy baja prevalencia de miopía en esta población. Futuros estudios que incluyan diversas poblaciones con alta prevalencia de astigmatismo elevado podrían contribuir a una mejor comprensión de los factores relevantes en la etiología de este rasgo.
Palabras clave: miopía, astigmatismo fuerte, prevalencia, Salta, Argentina.
Prevalência de alto astigmatismo na província de Salta, Argentina
RESUMO
Objetivo: Erros de refração são a principal causa de deficiência visual. Os dados de prevalência são fundamentais para o planejamento de estratégias de saúde visual, uma vez que a detecção e o tratamento precoces dos erros refrativos em crianças têm um papel fundamental no desenvolvimento normal da visão.
Métodos: Estudo transversal de base populacional, no qual participaram escolares de 4 a 15 anos, atendidos de março a novembro de 2014. Realizou-se autorefratometria sob cicloplegia e refração subjetiva. A miopia foi considerada como o erro refrativo para um equivalente esférico <-0,50 dioptrias e hipermetropia como> + 2,00 D. Para os fins deste estudo, o astigmatismo foi considerado igual ou superior a -2,00 dioptrias.
Resultados: A amostra foi composta por 1.852 crianças com 8,03 ± 2,57 anos, com variação de 4 a 15 anos, sendo 967 (52,2%) mulheres. Destes, 116 indivíduos (6,26%) tinham um equivalente esférico menor ou igual a -0,50 dioptrias e havia 111 (5,99%) indivíduos com um cilindro refrativo ≤ -2,00 dioptrias (limite -7,50 dioptrias). Na região de Seclantas (altas montanhas) a amostra foi composta por 157 crianças, das quais 20 (12,75%) apresentaram valores de astigmatismo no olho direito ≤ -2,00 dioptrias.
Conclusões: Uma alta prevalência de astigmatismo alto e uma prevalência muito baixa de miopia foram encontradas nesta população. Estudos futuros que incluam diversas populações com alta prevalência de astigmatismo elevado podem contribuir para um melhor entendimento dos fatores relevantes na etiologia desta característica.
Palavras chave: miopia, forte astigmatismo, prevalência, Salta, Argentina.
INTRODUCTION
Refractive errors are the first cause of visual impairment across the world1. Prevalence data are crucial for planning public health strategies, particularly in visual health, since early detection and treatment of refractive errors in children has a key role on normal vision development and learning. The principal objectives of health planning are to prevent the development of high myopia and refractive amblyopia, causes of avoidably visual acuity loss2-3.
Many studies have described the epidemiology of refractive errors worldwide. The distribution of its related vision impairment has shown interesting variations in different regions and countries4. Notwithstanding, there is scarce information about prevalence of refractive errors in children in Latin America5-7. This could be due to the fact that Latin American countries seldom allocate resources for these studies. Given that this region represents 10% of the world population, studies in Latin America can strongly contribute to the knowledge and understanding of the epidemiology of refractive errors. The purpose of this study was to evaluate the prevalence, type and severity of refractive errors in school-aged children in the province of Salta, located in the North West Region of Argentina.
MATERIALS AND METHODS
Study design, ethics and participants
This was a cross-sectional population based study, which involved school-children aged 4-15-year-old residents in Salta province, Argentina. Children were examined from March to November, 2014. The exams were part of a preventive campaign (20/20 Program), developed by the government of Salta province. This campaign schedules and provides visits by a trained ophthalmologist who travels by bus and stays for few days in suburban and rural locations for the examinations at local schools. The campaign provides ophthalmological attention and spectacle provision for those who meet the need.
This screening was approved by the local authorities of Salta. The study project was also submitted to the Ethics Committee of the Argentinian Council of Ophthalmology which stated that no approval was needed for this study. Two weeks before the ocular exam took place in each school an informed consent was sent as homework for the parents to allow and sign for the examination. All data were treated confidentially in accordance to the Declaration of Helsinki and Argentine laws. According to the 2010 population census Salta province has 311.090 primary and secondary students in 1096 schools8.
Settings and procedures
The ocular exam took place at the school buildings and consisted of several days of work at each of the 9 zones involved in this study, with mobile assessment tools. The children were examined by one ophthalmologist (RDD) who first tested visual acuity projecting a Snellen letters optotype chart (Rusner, Argentina) at 3 meters distance. The threshold for normal visual acuity was stablished at 7/10 and when a child did not reach this visual acuity in either eye, the child was further assessed with a cycloplegic exam. The cycloplegia was obtained with two drops of cyclopentolate 1% instilled five minutes apart after a drop of proparacaine 0,2% for topical anesthesia. After one hour, pupil dilation and absence of pupillary reflex were confirmed and objective refraction was obtained with an automatic refractometer (UNICOS, Korea). With this cycloplegic refractive error measurement, the day after pupil dilation, a subjective refraction was refined with a hand held bar retinoscope and neutralization with known trial lenses (WelchAllyn, USA) performed by the same trained ophthalmologist. After this the spectacles were prescribed and provided with adequate frames by technical personnel.
Main outcomes and statistical evaluation
The spherical equivalent refraction (SER) was calculated as the sphere + ½ the cylinder value. For the purpose of reporting prevalence of refractive error, the present study followed the protocol of Refractive Error Studies in Children and the recommendations of the International Myopia Institute9-10: myopia was considered as the spherical equivalent refractive error <-0,50 diopters (D), hyperopia as >+2.00 D, and the rest among -0.50 and +2.00 D were considered emmetropes. For the purpose of this study astigmatism was considered as that equal or greater than -2.00 diopters. Parametric values were expressed as mean, standard deviations and range. The data were recorded in an Excel spreadsheet and converted to SPSS database (SPSS version 15, SPSS Inc., Chicago, IL, USA).
RESULTS
The sample consisted of 1852 children aged 8.03 ± 2.57 years, range 4 to 15 years of whom 967 (52.2%) were females. The number of children in each studied location is given in Table 1. All locations except Zone 9 (Seclantas) were located in the neighborhoods of Salta city, in the valley of the river Rosario, at 1,152 meters altitude over sea level. Seclantas was located in the mountainside at an altitude of 3,000 meters over the sea level.
Table 1. Number of children in each studied location.
Number of subjects in each zone |
||
Zone |
n= |
% |
1 |
83 |
4.5% |
2 |
27 |
1.5% |
3 |
240 |
13.0% |
4 |
134 |
7.2% |
5 |
679 |
36.7% |
6 |
213 |
11.5% |
7 |
290 |
15.7% |
8 |
29 |
1.6% |
9 |
157 |
8.5% |
Total |
1852 |
100% |
The unaided visual acuity in decimal notation had a mean value of 0.91 ± 1.81 for the right eyes and left eyes, with no difference between them. The relative percentages of each visual acuity level are presented in Table 2.
Table 2. Relative percentages of visual acuity in decimals.
Visual acuity |
n= |
% |
Count fingers |
5 |
0.3% |
1·0 |
12 |
0.6% |
0·2 |
20 |
1.1% |
0·3 |
25 |
1.3% |
0·4 |
19 |
1.0% |
0·5 |
47 |
2.5% |
0·6 |
63 |
3.4% |
0·7 |
83 |
4.4% |
0·8 |
32 |
1.7% |
0·9 |
224 |
12.1% |
10·0 |
1322 |
71.4% |
There were 288 (15.5%) children in the sample who did not reach the 7/10 cut off for unaided visual acuity and were studied with cycloplegia. The mean cycloplegic refractive error was similar for both eyes (r = 0.86, p < 0.001) so only right eyes are reported here. The mean refractive error was virtually emmetropic for the right eyes, for example (spherical equivalent = 0.00 ± 2.15 diopters).
There were 116 subjects (6.26% of the whole sample) with myopic spherical equivalent lower or equal than -0.50 diopters (limit -9.81 diopters), and 102 (5.51% of the whole sample) with spherical equivalent greater than +0.50 diopters (limit +9.87 diopters). There were 111 (5.99%) subjects with refractive cylinder ≤ -2.00 diopters (limit -7.50 diopters). There was a high correlation between the refractive cylinder of the right and left eyes (r =0.80, p <0.001). The correlation between visual acuity and refractive astigmatism in figure 1 (r = 0.86, p < 0.001) shows that a cut point of -2.00 diopters of astigmatism represents an uncorrected visual acuity of 0.6 points, the usual limit for detecting relevant refractive error11.
Figure 1. Correlation between visual acuity and astigmatism of the right eyes.
As there was an important prevalence of high simple myopic astigmatism, some subjects looked like biased myopes with not true negative spherical equivalent (for example a -2.00 diopters simple myopic astigmatism classifies as a -1.00 diopters spherical equivalent myopic subject). Excluding these simple myopic astigmatic subjects, out of the mentioned 116 subjects with myopic spherical equivalent, only 49 had some spherical component ≤ than -1.00 diopter. This leads to an estimated prevalence of true myopic spherical equivalent in the whole sample of 3.61%.
Out of the 111 subjects with cylinder ≤ than -2.00 diopters, there were 44 (2.37% of the sample) with spherical equivalent ≤ than -0.50 diopters (simple myopic astigmatism), and 41 (2.21%) with spherical equivalent ≥ than +0.50 diopters (simple hyperopic astigmatism). The rest were mixed astigmatisms.
There were 64 subjects with an anisometropia of 1 diopter or more in the whole sample (3.45%) and 70 with a difference of 1 diopter or more between the astigmatic value of both eyes (anisoastigmatism 3.78%).
In the Seclantas zone the sample comprised 157 children, of whom 20 (12.75%) had astigmatic values in the right eyes ≤ than -2.00 diopters. There were 46 (29.3%) children with myopic spherical equivalent ≤ than -0.50 diopters, but as most were simple astigmats, only 14 (8.9%) had a myopic sphere ≤ than -1.00 D.
DISCUSSION
This school-based study evaluated the prevalence, severity, and type of refractive errors of children in the province of Salta, Argentina in 2014. This is the largest report in Argentina that has studied refractive errors under cycloplegic refraction in school-aged children. Our study found that the overall prevalence rate of high astigmatism ≤ -2.00 diopters was 5.99%. Regarding the type of astigmatism, with-the-rule astigmatism was the most prevalent type, in concordance with the majority of reports of astigmatism in school-aged children12.
The prevalence of astigmatism has been studied in different parts of the world and estimates of astigmatic prevalence seem to vary depending on the ancestral continental origin of examined populations4. Overall, studies including children of East Asian and Indigenous American ancestry report a relatively high prevalence of high astigmatism compared with studies that were conducted in individuals of mostly European, African and West Asian ancestry (Iran, Turkey, India) (Tables 3 and 4).
For example, in 1977 a seminal study by Mohindra & Nagaraj compared the prevalence of high astigmatism of -3.00 or more diopters in groups of more than 300 first level schoolchildren of Native Canadian (Northern Saskatchewan), Zuni and Navajo ancestry vs. European Canadians, finding that the prevalence of these high levels of astigmatism reached 27.0% in members of the Zuni tribe, 12.8% in Navajo people, 7.0% in Native Canadians (Northern Saskatchewan) and only 1.6% in European Canadians13. Additionally, a study conducted in a random sample of children from the city of Santiago de Chile has also described elevated high astigmatism prevalence in South America7.
The North West Argentina region, where Salta is located, has been described as the region with the largest average proportion of Indigenous American ancestry in the country, ranging from 65% to 72% according to different studies14-15.
The current results are, therefore, consistent with previous reports of higher prevalence of high astigmatism in studies that include individuals of Indigenous American origin (Tables 3-4). Noteworthy, there is conflicting evidence regarding this issue, since environmental factors have also been proposed as possible determinants or triggers for the development of astigmatism16-17. It is important to highlight that studies on the influence of genetic and environmental factors in astigmatism have been conducted in individuals of mostly European origin, and do not differentiate high or low degrees of astigmatism18-19. We believe that, as in the case of high myopia, high astigmatism could be segregated from low astigmatism. High amounts of astigmatism are more important because they are the ones related to the development of amblyopia20-21. And also low amounts of astigmatism (-0.75 or -1.00 diopters) are present in a high proportion of most populations of children, while the figures drop down essentially when a cut point of -2.00 diopters is used. There has not been a consensus of what cut point may be adequate for considering high astigmatism. For our study we propose -2.00 diopters based on the drop down of the prevalence found at this particular cut point.
Table 3. Prevalence of astigmatism ≤ -2.00 in different studies.
Country |
n= |
Location |
Age (years) |
% |
USA Arizona (Aboriginals)22 |
1235 |
Tohono O’Odham |
6-8 |
21.47% |
Chile23 |
5303 |
La Florida |
5-15 |
10.42% |
Korea (*<-2,00)24 |
7486 |
National Healt Survey |
5-19 |
9.30% |
Ecuador25 |
1564 |
Quito (Andean) |
5-6 |
7.89% |
Singapore26 |
1028 |
Singapore |
7-9 |
6.64% |
China27 |
1496 |
Hong Kong |
6-8 |
6.30% |
Argentina (present study) |
1852 |
Salta |
5-15 |
5.99% |
China28 |
4364 |
Guangzhou |
5-15 |
5.90% |
Taiwan29 |
11175 |
Taiwan |
7-18 |
5.10% |
Alaskan Eskimos (*<-2,00)30 |
1848 |
Norton Sound |
- |
3.50% |
Malaysia31 |
4634 |
Gombak |
7-15 |
3.40% |
Iran32 |
1033 |
Tehran |
5-15 |
3.38% |
Ireland33 |
1623 |
Dublin |
6-13 |
3.32% |
Brazil34 |
2825 |
São Paulo |
8-14 |
2.05% |
India35 |
6447 |
New delhi |
5-15 |
1.20% |
South Africa36 |
4890 |
Durban |
5-15 |
1.10% |
Turkey37 |
21062 |
Diyarbakir |
6-14 |
0.90% |
Nepal38 |
5067 |
Mechi zone |
5-15 |
0.88% |
Pakistan39 |
45122 |
Rawalpindi |
5-16 |
0.06% |
Table 4. Prevalence of astigmatism ≤ -1.50 diopters in different studies.
Study |
n= |
Ethnicity |
Age (years) |
Prevalence |
Mohindra40 |
- |
Zuni Aboriginals (Inbred) |
6-8 |
27.00% |
China (YiWu)41 |
4801 |
East Asians |
4-12 |
14.20% |
Ecuador25 |
1564 |
Quito (Andean) |
5-6 |
13.20% |
Mohindra40 |
- |
Navajo Aboriginals |
6-8 |
12.80% |
STARS (Singapore)42 |
530 |
South Asians |
5-6 |
11.30% |
Argentina (Salta) |
1852 |
Andean (present study) |
5-15 |
7.29% |
Mohindra40 |
- |
Canadian Aboriginals |
6-8 |
7.00% |
Australia (Sydney)43 |
129 |
South Asians |
12 |
6.30% |
China (Anyang)44 |
1783 |
South Asians |
12 |
5.90% |
Australia (Sydney)43 |
352 |
East Asians |
12 |
4.90% |
Iran32 |
4354 |
Middle Eastern |
≥5 |
4.30% |
Australia (Sydney)43 |
166 |
Middle Eastern |
12 |
3.70% |
Australia (Sydney)43 |
1407 |
Caucasians |
12 |
1.70% |
Mohindra40 |
- |
Canadian Caucasians |
6-8 |
1.60% |
Based on the results of this study as well as on previous reports of prevalence in East Asian and Indigenous American populations, we hypothesize that high astigmatism might be partly triggered by a genetic variant or variants associated with ancestral East Asian and Indigenous American population components. Consistent with this hypothesis, among 157 children from our study who were from the Seclantas zone, 20 (12.75%) had astigmatic values in the right eyes ≤ -2.00 diopters, almost doubling the mean value of the overall study sample. Seclantas is located far from the capital city, in the mountainside, at an altitude of 3000 meters over the sea level, and its relative isolation has contributed to lower levels of European admixture in the population, similarly to the Zuni people. The possible genetic contribution to high astigmatism in these populations has yet to be demonstrated in future studies.
Strengths of the study include the large sample size compared to other studies in the region, the fact that it was population based (school-based) and that it was performed with cycloplegic refractions. A possible limitation is that no other information, such as ethnicity, time spent at school and outdoors, or use of spectacles was gathered. Future studies in the zone will include myopia risk factors.
We also want to address the issue of the low prevalence of myopia in this sample of schoolchildren. There are some studies under way in Latin America (Magnetto et al. and Zeman et al., both in preparation) showing that the prevalence of myopia in schoolchildren is relatively low. It would be interesting to gather information about the academic achievement and outdoor exposure of children in these countries to understand why the increasing prevalence of myopia that has been reported in most parts of the world has not yet been observed in Latin America. The data for the current study were gathered in 2014 as part of refractive errors screening efforts led by our group. Similar data could be available as the screening for refractive errors in schools is a common ophthalmological practice all over the country. Our group hopes that the records of these abundant screenings may be systematically collected and shared, contributing to epidemiologic research in refractive error.
REFERENCES
1. WHO. Magnitude and causes of visual impairment. Fact Sheet 282, 2004.
2. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol 2012; 96: 614-618.
3. Wolffsohn JS, Flitcroft DI, Gifford KL et al. IMI: myopia control reports overview and introduction. Invest Ophthalmol Visual Sci 2019; 60: M1-M19.
4. Hashemi H, Fotouhi A, Yekta A et al. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol 2017; 30: 3-22.
5. Lira RPC, Espirito Santo IF do, Astur GLV et al. Refractive error in school children in Campinas, Brazil. Arq Bras Oftalmol 2014; 77: 203-204.
6. Thorn F, Cruz AAV, Machado AJ, Carvalho RAC. Refractive status of indigenous people in the northwestern Amazon region of Brazil. Optom Vis Sci 2005; 82: 267-272.
7. Maul E, Barroso S, Munoz SR et al. Refractive error study in children: results from La Florida, Chile. Am J Ophthalmol 2000; 129: 445-454.
8. Argentina. Instituto Nacional de Estadística y Censos (INDEC). Censo nacional 2010 [National census 2010]. Available: https://www.indec.gob.ar/indec/web/Nivel4-Tema-2-41-135
9. Flitcroft DI, He M, Jonas JB et al. IMI: defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci 2019; 60: M20-M30.
10. Negrel AD, Maul E, Pokharel GP et al. Refractive Error Study in Children: sampling and measurement methods for a multi-country survey. Am J Ophthalmol 2000; 129: 421-426.
11. Leone JF, Mitchell P, Morgan IG et al. Use of visual acuity to screen for significant refractive errors in adolescents: is it reliable? Arch Ophthalmol 2010; 128: 894-899.
12. Read SA, Collins MJ, Carney LG. A review of astigmatism and its possible genesis. Clin Exp Optom 2007; 90: 5-19.
13. Mohindra I, Nagaraj S. Astigmatism in Zuni and Navajo indians. Am J Optom Physiol Opt 1977; 54: 121-124.
14. Avena S, Via M, Ziv E et al. Heterogeneity in genetic admixture across different regions of Argentina. PLoS One 2012; 7: e34695.
15. Wang S, Ray N, Rojas W et al. Geographic patterns of genome admixture in Latin American Mestizos. PLoS Genet 2008; 4: e1000037.
16. Read SA, Vincent SJ, Collins MJ. The visual and functional impacts of astigmatism and its clinical management. Ophthalmic Physiol Opt 2014; 34: 267-294.
17. Read SA, Collins MJ, Carney LG. A review of astigmatism and its possible genesis. Clin Exp Optom 2007; 90: 5-19.
18. Valluri S, Minkovitz JB, Budak K et al. Comparative corneal topography and refractive variables in monozygotic and dizygotic twins. Am J Ophthalmol 1999; 127: 158-163.
19. Lee KE, Klein BE, Klein R, Fine JP. Aggregation of refractive error and 5-year changes in refractive error among families in the Beaver Dam Eye Study. Arch Ophthalmol 2001; 119: 1679-1685.
20. Dobson V, Miller JM, Harvey EM, Mohan KM. Amblyopia in astigmatic preschool children. Vision Res 2003; 43: 1081-1090.
21. Brown SA, Weih LM, Fu CL et al. Prevalence of amblyopia and associated refractive errors in an adult population in Victoria, Australia. Ophthalmic Epidemiol 2000; 7: 249-258.
22. Twelker JD, Miller JM, Sherrill DL, Harvey EM. Astigmatism and myopia in Tohono O’odham Native American children. Optom Vis Sci 2013; 90: 1267-1273.
23. Maul E, Barroso S, Munoz SR et al. Refractive error study in children: results from La Florida, Chile. Am J Ophthalmol 2000; 129: 445-454.
24. Rim TH, Kim SH, Lim KH et al. Refractive errors in Koreans: The Korea National Health and Nutrition Examination Survey 2008-2012. Korean J Ophthalmol 2016; 30: 214-224.
25. Virgili G, Angi M, Heede S et al. PowerRefractor versus Canon R-50 autorefraction to assess refractive error in children: a community-based study in Ecuador. Optom Vis Sci 2007; 84: 144-148.
26. Tong L, Saw SM, Carkeet A et al. Prevalence rates and epidemiological risk factors for astigmatism in Singapore school children. Optom Vis Sci 2002; 79: 606-613.
27. Yam JC, Tang SM, Kam KW et al. High prevalence of myopia in children and their parents in Hong Kong Chinese population: the Hong Kong Children Eye Study. Acta Ophthalmol 2020. doi:10.1111/aos.14350
28. He M, Zeng J, Liu Y et al. Refractive error and visual impairment in urban children in southern china. Invest Ophthalmol Vis Sci 2004; 45: 793-799.
29. Shih YF, Hsiao CK, Tung YL et al. The prevalence of astigmatism in Taiwan schoolchildren. Optom Vis Sci 2004; 81: 94-98.
30. van Rens GHBatholomeus. Ophthalmologic findings among Alaskan Eskimos of the Norton Sound and Bering Straits region [thesis]. Nijmegen (Netherlands), 1988. Katholieke Universiteit te Nijmegen.
31. Goh PP, Abqariyah Y, Pokharel GP, Ellwein LB. Refractive error and visual impairment in school-age children in Gombak District, Malaysia. Ophthalmology 2005; 112: 678-685.
32. Hashemi H, Fotouhi A, Mohammad K. The age- and gender-specific prevalences of refractive errors in Tehran: the Tehran Eye Study. Ophthalmic Epidemiol 2004; 11: 213-225.
33. Harrington SC, Stack J, Saunders K, O’Dwyer V. Refractive error and visual impairment in Ireland schoolchildren. Br J Ophthalmol 2019; 103: 1112-1118.
34. Salomão SR, Cinoto RW, Berezovsky A et al. Prevalence and causes of visual impairment in low-middle income school children in Sao Paulo, Brazil. Invest Ophthalmol Vis Sci 2008; 49: 4308-4313.
35. Murthy GVS, Gupta SK, Ellwein LB et al. Refractive error in children in an urban population in New Delhi. Invest Ophthalmol Vis Sci 2002; 43: 623-631.
36. Naidoo KS, Raghunandan A, Mashige KP et al. Refractive error and visual impairment in African children in South Africa. Invest Ophthalmol Vis Sci 2003; 44: 3764-3770.
37. Caca I, Cingu AK, Sahin A et al. Amblyopia and refractive errors among school-aged children with low socioeconomic status in southeastern Turkey. J Pediatr Ophthalmol Strabismus 2013; 50: 37-43.
38. Pokharel GP, Negrel AD, Munoz SR, Ellwein LB. Refractive Error Study in Children: results from Mechi Zone, Nepal. Am J Ophthalmol 2000; 129: 436-444.
39. Gull A, Raza A. Visual screening and refractive errors among school aged children. J Rawalpindi Med College 2014; 18: 97-100.
40. Mohindra I, Nagaraj S. Astigmatism in Zuni and Navajo indians. Am J Optom Physiol Opt 1977; 54: 121-124.
41. Wang J, Cheng QE, Fu X et al. Astigmatism in school students of eastern China: prevalence, type, severity and associated risk factors. BMC Ophthalmol 2020; 20: 155.
42. Dirani M, Chan YH, Gazzard G et al. Prevalence of refractive error in Singaporean Chinese children: the strabismus, amblyopia, and refractive error in young Singaporean Children (STARS) Study. Invest Ophthalmol Vis Sci 2010; 51: 1348-1355.
43. Huynh SC, Kifley A, Rose KA et al. Astigmatism in 12-year-old Australian children: comparisons with a 6-year-old population. Invest Ophthalmol Vis Sci 2007; 48: 73-82.
44. Li H, Li SM, Liu LR et al. Astigmatism and its components in 12-year-old Chinese children: the Anyang Childhood Eye Study. Br J Ophthalmol 2019; 103: 768-774.