ORIGINAL ARTICLES
Development of a frame adaptation for myopia control spectacles
Guillermo Saraccoa, Matías Acerbib, Martín de Tomásc, Gabriel Martínc, Rafael Iribarrenc-e
a Saracco Optical Center, Buenos Aires, Argentina.
b Foucault Optical Center, Buenos Aires, Argentina.
c Novar, Miami, Estados Unidos.
d Drs. Iribarren Eye Consultants, Buenos Aires, Argentina.
e Retina Foundation, Buenos Aires, Argentina.
Received: April 4th, 2025.
Approved: May 20th, 2025.
Corresponsal author
Dr. Guillermo Saracco
Juncal 821
Buenos Aires, Argentina.
+54 (911) 5001-3054.
gsaracco19@gmail.com
Oftalmol Clin Exp (ISSNe 1851-2658)
2025; 18(2): e195-e201.
https://doi.org/10.70313/2718.7446.v18.n2.423
Acknowledgments
Novar (Miami, USA) company provided de MyofixTM lenses and Usual (Buenos Aires, Argentina) provided the frames.
Financial disclosures
Martín de Tomás, Gabriel Martín and Rafael Iribarren work in Novar company. The devices tested in this work are not currently under any patent.
Abstract
Purpose: To develop a specific frame adaptation device for myopia control spectacles and conduct its first experimental test.
Methods: Two plastic devices were created, each with a central opening to align with the eye. These are used in front of spectacle frames to verify that the optical treatment zone is correctly positioned. One device adheres directly to the frame and can be easily removed; the other one is handheld and used to test the centering of the 33 mm annular treatment zone. Both devices were tested on a voluntary myopic female subject to evaluate alignment and positioning of optical treatment areas using MyofixTM peripheral plus defocus lenses (developed by Novar, Argentina), which feature a 9 mm central distance vision zone and a peripheral full-diameter treatment zone.
Results: Five different frames were evaluated. The pupil’s position was determined for each frame. With the devices centered on the pupil, the four frame edges (nasal, superior, temporal, and inferior) were assessed for inclusion of the treatment area. Proper centering ensured accurate evaluation of lens alignment. Only two of the five frames allowed full inclusion of the treatment zone within the frame boundaries. For optimal calibration during lens blocking, the devices must be centered as precisely as possible.
Conclusion: Two simple and practical devices were developed to aid in the centering of defocus myopia control spectacles. These tools may be easily implemented in clinical practice in the future.
Keywords: Optical frame adaptation, spectacles centering, myopia control spectacles, myopia.
Desarrollo de una montura de adaptación para las gafas de control de la miopía
Resumen
Objetivo: Desarrollar un dispositivo de adaptación de montura específico para gafas de control de la miopía y realizar su primera prueba experimental.
Materiales y métodos: Se diseñaron dos dispositivos plásticos con una abertura central para alinear con el ojo, utilizados frente a las monturas para verificar que la zona óptica de tratamiento esté bien posicionada. Uno se adhiere directamente a la montura y es removible; el otro se sostiene manualmente para comprobar el centrado de la zona anular de tratamiento de 33 mm. Ambos se probaron en una paciente miope voluntaria para evaluar la alineación de zonas ópticas usando lentes Myofix® (Novar, Argentina), que poseen una zona central de 9 mm para visión lejana y una zona periférica completa de tratamiento.
Resultados: Se evaluaron cinco monturas diferentes. Se determinó la posición pupilar en cada una. Con los dispositivos centrados en la pupila se evaluaron los bordes nasal, superior, temporal e inferior para verificar la inclusión de la zona de tratamiento. El centrado adecuado permitió una evaluación precisa. Solo dos de las cinco monturas aseguraron la inclusión completa de la zona óptica dentro de los límites del armazón. Para una calibración precisa en el bloqueo de la lente, los dispositivos deben centrarse lo más exactamente posible.
Conclusiones: Se desarrollaron dos dispositivos simples y útiles para facilitar el centrado de lentes desenfocadas para control de miopía. Podrían incorporarse fácilmente en la práctica clínica en el futuro.
Palabras clave: adaptación de montura óptica, centrado de gafas, gafas de control de miopía, miopía.
Desenvolvimento de uma armadura adaptável para óculos de controle de miopia
Resumo
Objetivo: Desenvolver um dispositivo específico de adaptação de armação para óculos de controle de miopia e realizar seu primeiro teste experimental.
Materiais e métodos: Dois dispositivos plásticos com abertura central foram projetados para alinhamento com o olho e usados na frente das armações para verificar se a zona de tratamento óptico estava corretamente posicionada. Um adere diretamente à armação e é removível; o outro é segurado manualmente para verificar a centralização da zona de tratamento anular de 33 mm. Ambos foram testados em um paciente míope voluntário para avaliar o alinhamento da zona óptica usando lentes Myofix® (Novar, Argentina), que possuem uma zona central de 9 mm para visão à distância e uma zona de tratamento periférica completa.
Resultados: cinco armações diferentes foram avaliadas. A posição pupilar foi determinada em cada uma delas. Com os dispositivos centralizados na pupila, as bordas nasal, superior, temporal e inferior foram avaliadas para verificar a inclusão da zona de tratamento. A centralização adequada permitiu uma avaliação precisa. Apenas duas das cinco armações garantiram a inclusão completa da zona óptica dentro dos limites da armação. Para uma calibração precisa do bloco de lentes, os dispositivos devem ser centralizados com a maior precisão possível.
Conclusões: Dois dispositivos simples e úteis foram desenvolvidos para facilitar a centralização de lentes desfocadas para o controle da miopia. Eles poderão ser facilmente incorporados à prática clínica no futuro.
Palavras-chave: adaptação de armações ópticas, centralização de óculos, óculos para controle da miopia, miopia.
Introduction
In recent years the industry has developed many spectacles designed to arrest myopia progression1-4. The first one to be presented as early as 2019 (published in 2020), involves a distance central area 9 mm diameter wide and a treatment area 33 mm diameter wide1. When this design was developed, it was known that annular rings with positive add leaving a central 3 mm diameter for distance correction in contact lenses were adequate for controlling myopia progression5. A 9 mm diameter central hole for distance vision at the spectacle plane also resulted in arresting myopia progression in the first clinical trial of spectacles for myopia control1. At later time it came to be known that the parafoveal zone around 6º to 12º from the ocular axis is the zone responsible for detecting growth signals in the eye6-76. This zone is the same that in genetic high myopia (probably involving metabolic inherited defects in the signal that governs eye growth) produces a posterior staphyloma involving the 20º diameter around the fovea, showing that it is the zone affected by excessive ocular growth8.
With OCT fundus photographs, our group has shown that the retinal area covered by the small lenslets in the original design falls approximately in this same annular ring around the fovea9-10 which is responsible for detecting ocular growth signals. Our team has also shown that vertex distance, which depends on the anthropometric parameters of the face and the correct election of frames, has crucial importance for making the treatment zone reach this sector of the retina11.
Considering the relevance that these spectacles must be accurately centered so the treatment area falls inside the elected frame and is projected to the retinal plane, our purpose was to developed a frame adaptation specific for the MyofixTM spectacle12, to ensure these treatment zones are correctly centered for effective myopia control.
Material and methods
An experimental set up study was developed. Two plastic devices were designed to aid in the selection, adaptation, and calibration of myopia control spectacles. These devices, used to align and verify the positioning of the optical treatment zones, were tested with the MyofixTM peripheral plus add defocus lenses developed in Argentina by Novar laboratory12. This spectacle has a central circular zone for distance correction 9 mm wide and a full peripheral defocus area with plus add. It is conceived from studies with DIMS1 and HAL13 spectacles in which the treatment area involves a greater circular zone 33 mm diameter wide around the central 9 mm zone for distance vision. The plastic devices developed for this study feature a central clear area to allow visualization of the centered eye, ensuring that at least a 33 mm diameter for the treatment zone aligns properly within the frame.
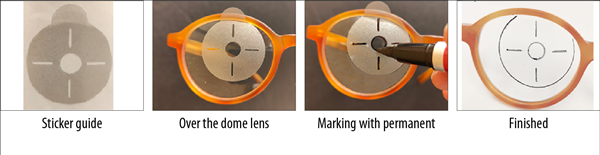
These two devices were developed to help in maintaining this area in the frames with the eyes centered. The two devices are plastic made and have central zones free for looking at the centered eye and must be applied in front of the frames to check that the treatment area falls inside the frames (Fig. 1). The first device is adherent to the frame and can be easily removed. The second device can be sustained by hand to test the centering of the 33 mm annular zone for treatment area (Fig. 2).
Figure 1. Device of adherent plastic attached alone to the left and attached to the frames middle, and drawn for centering to the right.
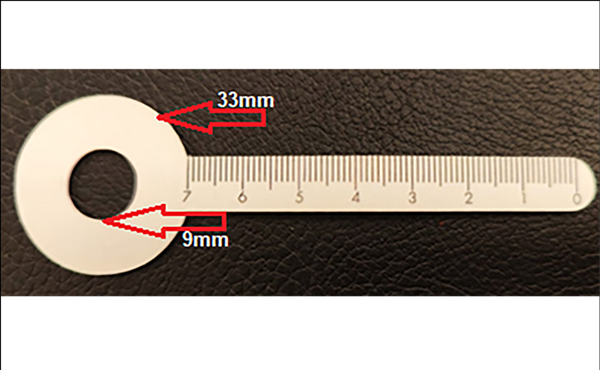
Figure 2. Second device, plastic ruler with same dimensions as device 1.
To perform the experimental tests on a real user a young myopic female was volunteer for this study. The subject and both parents filled informed consent for the publication of her photographs. Several frames (Usual, Buenos Aries, Argentina) were tested for adaptation with these two devices until the correct one which would be aesthetical for the subject was elected for MyofixTM spectacles prescription and adaptation. Refractive error was measured in Drs. Iribarren Eye Consultants office (Buenos Aires, Argentina). Both subjective and objective refractions after cycloplegia with cyclopentolate were measured (two drops 5 minutes apart and after 45 minutes). The refractive examination included visual acuity assessment with full correction, intraocular pressure with Goldman tonometer, inspection of the outer eye with slit lamp and fundus observation under Schepens when the pupil was dilated. The auto-refractometry unit used for the objective refraction was a Huvitz HRK 6000 autokeratometer (Huvitz, South Korea). Frame election took place one week after the refractive examination and was done in Saracco Optical Lab (Buenos Aries, Argentina).
Results
The subject was an eleven year old girl with family history of high myopia in the mother line who has been under treatment with atropine 0.01% and lifestyle changing habits for 5 years. With age of onset at 6 years old, she had a first prescription -1.50 diopters in both eyes. After 5 years of treatment with atropine her refraction was both eyes -3.50 diopters. During the last year she has had bad compliance with the drops when changing from mother putting the drops to put them on her own and has progressed to -4.25 sphere both eyes. The patient uses spectacles full day so it was suggested to use myopia control spectacles12 (MyofixTM, Novar, Miami, USA), and continue the drop treatment with good compliance.
At the optical store five different frames were tested (Figs. 3 & 4). The position of the patient’s pupil was established for each frame. With the two type of devices centered in the pupil, the 4 edges of the frame (nasal, superior, temporal and inferior) could be checked for inclusion of treatment area inside the frame. By centering the pupil using the developed devices, the inclusion of the treatment area within each frame was assessed. The most appropriate frame was determined according to the image of the devices falling as much as possible in the center of the frame for accurate calibration of the block of the lens. Out of the five frames, only two ensured that the entire optical treatment zone was enclosed within the frame.
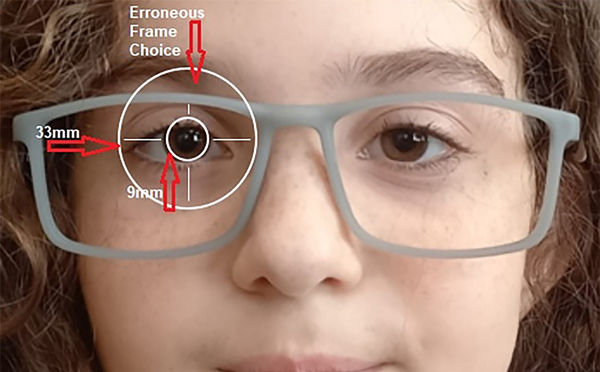
Figure 3. Projection of device placed at the center of the pupil to verify that the treatment area fits within the frame when centered.

Figure 4. (A) Device II located over the frames fit in the face to check correct centering. (B-F) Different frames fit in the young girl face to test centering and aesthetics balancing for the most suitable.
Discussion
Considering myopia control spectacles designs, in order for the 33 mm optical treatment zone to be completely inside the elected frame, the distance from center of the pupil to each of the edges of the frame must be at least 16.5 mm7. This can be simply checked with any of the two devices developed by our research team. For effective myopia control, the 33 mm optical treatment zone must fit entirely within the selected frame14-15 . This method ensures the lenses are accurately centered, optimizing the effectiveness of myopia control. In this study, the importance of selecting the correct frame for myopia control spectacles was highlighted, as these spectacles need precise centration to ensure their efficacy. Proper alignment of the treatment and distance zones within the frame is crucial to achieve effective myopia control. By carefully selecting frames and utilizing these calibration devices, practitioners can enhance the efficacy of myopia control spectacles, ensuring patients receive the full therapeutic benefit of the treatment.
If an inappropriate frame is selected, the 33.0 mm treatment area may not be completely enclosed within the frame. This misalignment can lead to uneven distribution of the optical treatment, possibly reducing its effectiveness in controlling myopia progression. This misalignment compromises the therapeutic benefit, potentially resulting in suboptimal control of myopia progression. An incorrect frame choice can also cause visual discomfort and strain. If the distance zones are not correctly centered, it may lead to issues such as blurred vision, double vision, or difficulty in focusing, which can cause discomfort for the wearer.
A poor fit in the frames and the resulting ineffective treatment can lead to dissatisfaction among patients, who may not see the expected arresting in their condition. This dissatisfaction could affect compliance with wearing the spectacles, further diminishing the benefits of the treatment. To avoid these negative outcomes, the study emphasizes the necessity of choosing frames that allow the entire 33 mm treatment zone to be correctly centered within the frame. The developed devices assist in ensuring the frame choice provides at least 16.5 mm distance from the center of the pupil to each edge of the frame, thereby optimizing the positioning of the myopia control lenses. In our practice we have noticed that both devices have some application. The first handheld device helps in electing the correct frame that when centered includes the peripheral treatment zone. The second (stick-on device) is important once the lenses have been calibrated in the frames to check for correct centering when the patient comes to fetch up the spectacles. Once delivered, the stick-on device is retired from the lenses.
Conclusion
The facts addressed in the present study have seldom been considered in clinical trials with this type of spectacles, and surely may be important in real life experiences when these devices become the standard of treatment for myopia control. The development of better tools for centering should be a topic of research.
References
1. Lam CSY, Tang WC, Tse DY, Lee RPK, Chun RKM, Hasegawa K, Qi H, Hatanaka T, To CH. Defocus incorporated multiple segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol 2020; 104: 363-368. doi:10.1136/bjophthalmol-2018-313739.
2. Lupon M, Nolla C, Cardona G. New designs of spectacle lenses for the control of myopia progression: a scoping review. J Clin Med 2024; 13(4): 1157. doi:10.3390/jcm13041157.
3. Zhang XJ, Zaabaar E, French AN et al. Advances in myopia control strategies for children. Br J Ophthalmol 2025; 109(2): 165-176. doi:10.1136/bjo-2023-323887.
4. Li X, Huang Y, Liu C, Chang X, Cui Z, Yang Q, Drobe B, Bullimore MA, Chen H, Bao J. Myopia control efficacy of spectacle lenses with highly aspherical lenslets: results of a 5-year follow-up study. Eye Vis (Lond) 2025; 12: 10. doi:10.1186/s40662-025-00427-3.
5. Anstice NS, Phillips JR. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology 2011; 118(6):1152-1161. doi:10.1016/j.ophtha.2010.10.035.
6. Panorgias A, Aigbe S, Jeong E, Otero C, Bex PJ, Vera-Diaz FA. Retinal responses to simulated optical blur using a novel dead leaves ERG stimulus. Invest Ophthalmol Vis Sci. 2021;62(10):1. doi:10.1167/iovs.62.10.1
7. Swiatczak B, Scholl HPN, Schaeffel F. Retinal „sweet spot“ for myopia treatment. Sci Rep 2024; 14(1): 26773. doi:10.1038/s41598-024-78300-x
8. Ohno-Matsui K, Wu PC, Yamashiro K, et al. IMI pathologic myopia. Invest Ophthalmol Vis Sci 2021; 62(5): 5. doi:10.1167/iovs.62.5.5 [errata corrected in: Invest Ophthalmol Vis Sci 2021 Jun 1; 62(7): 17. doi: 10.1167/iovs.62.7.17].
9. de Tomas M, Szeps A, Martin G, Suarez JM, Atchison DA, Rozema JJ, Iribarren R. Retinal shadows produced by myopia control spectacles. Ophthalmic Physiol Opt 2024; 44(1): 214-218. doi:10.1111/opo.13228.
10. Ho A, Feng L, Rozema JJ, Atchison DA. Retinal shadows of multisegment lenses in fundus imaging. Ophthalmic Physiol Opt Published online May 14, 2025. doi:10.1111/opo.13524.
11. de Tomas M, Szeps A, Martín G, Saracco G, Lanca C, Iribarren R. Effect of vertex distance in the treatment area of myopia control spectacles. Oftalmol Clin Exp 2024; 17(4): e547-e553. doi:10.70313/2718.7446.v17.n04.367.
12. de Tomas M, Kotklik C, Szeps A, Impagliazzo R, Iribarren R. New spectacles for myopia control. Oftalmol Clin Exp 2022; 15(2): 244-247. doi:10.70313/2718.7446.v15.n2.159.
13. Sankaridurg P, Weng R, Tran H et al. Spectacle lenses with highly aspherical lenslets for slowing myopia: a randomized, double-blind, cross-over clinical trial: parts of these data were presented as a poster at the Annual Research in Vision and Ophthalmology meeting, 2022. Am J Ophthalmol 2023; 247: 18-24. doi:10.1016/j.ajo.2022.10.021.
14. Schmidt DC, Hvid-Hansen A, Jacobsen N, Jakobsen TM, Larsen PM, Lindblad KK, Moller F, Slyngborg A, Subhi Y, Kessel L. Efficacy of interventions for myopia control in children: a systematic review with network meta-analyses. Acta Ophthalmol Published online April 11, 2025. doi:10.1111/aos.17496.
15. Sarkar S, Khuu S, Kang P. A systematic review and meta-analysis of the efficacy of different optical interventions on the control of myopia in children. Acta Ophthalmol. 2024; 102(3): e229-e244. doi:10.1111/aos.15746.