
ORIGINAL ARTICLES
Retinal neovascularization in ocular toxoplasmosis
Marcelo Rudzinskia-c, Ariel Schlaend,e, Macarena Chenlof, Cristóbal Coutod, Daniel Colomberog,h
aCátedra de Oftalmología, Universidad Católica de las Misiones, Posadas, Misiones, Argentina.
bConsultorio de uveítis y glaucoma, Marcelo Rudzinski Oftalmología, Oberá, Misiones, Argentina.
cConsejo Nacional de Investigaciones Científicas y Técnicas (CONICET), Buenos Aires, Argentina.
dDepartmento de Oftalmología, Hospital de Clínicas José de San Martín, Universidad de Buenos Aires, Argentina.
eDepartmento de Oftalmología, Hospital Universitario Austral, Buenos Aires, Derqui-Pilar, Argentina.
fServicio de Oftalmología, Hospital Escuela de Agudos “Ramón Madariaga”, Posadas, Misiones, Argentina.
gOftalmología Global, Rosario, Santa Fe, Argentina.
hDepartmento de Oftalmología, Universidad Nacional de Rosario, Rosario, Santa Fe, Argentina,
Oftalmol Clin Exp (ISSNe 1851-2658)
2024; 17(1): eXX-eXX.
Abstract
Purpose: To establish the frequency and clinical characteristics of retinal neovascularization (RN) as a complication of ocular toxoplasmosis (OT). Further, to report the most frequent approach of RN treatment used in OT patients.
Methods: A retrospective study was performed, reviewing clinical records of patients with diagnosis of OT from four tertiary referral uveitis centers, distributed in 3 different regions of Argentina. Collected data included best corrected visual acuity at presentation and that corresponding to the last examination, retinal location and extension of the toxoplasmic lesion and that of the retinal neovessels, treatment of the retinal neovascularization and retinal complications.
Results: A total of 550 records of patients with OT were reviewed, and 19 patients who developed RN were included. The frequency of RN in OT patients from Argentina was 3.16%. RN frequency was higher in OT patients from Misiones (5.33%) and almost unobserved in Buenos Aires (0.66%) (p=0.018). OT patients from Misiones developed RN in zone 2 while RN in OT patients from Santa Fe had a more peripheral location (p=0.016). Laser photocoagulation was the most frequent form of RN treatment in OT patients. Intravitreal bevacizumab for RN treatment could not induce complete involution of retinal neovessels.
Conclusions: RN in OT patients is an infrequent clinical presentation in Argentinian patients. Its frequency is higher in Misiones and Santa Fe than in Buenos Aires. Laser photocoagulation is the most frequent form of RN treatment in OT patients from Argentina.
Keywords: retinal neovascularization, ocular toxoplasmosis, laser photocoagulation, bevacizumab, Argentina.
Neovascularización retinal en toxoplasmosis ocular
Resumen
Objetivo: Determinar la frecuencia de neovascularización retinal (NR) y las características clínicas oculares de los pacientes con toxoplasmosis ocular (TO) que desarrollan esta complicación. Adicionalmente describir la forma de tratamiento más utilizada en Argentina en casos de NR en pacientes con TO.
Materiales y métodos: Se realizó un estudio clínico retrospectivo donde se revisaron historias clínicas de pacientes con toxoplasmosis de cuatro centros de referencia de uveítis de 3 regiones del país. Los datos analizados de las historias clínicas fueron agudeza visual al momento de la primera y última consulta, localización y extensión de la lesión retinal y del área de neovascularización, tratamiento de la NR y complicaciones retinales. Resultados: Se revisó un total de 550 historias clínicas de pacientes con toxoplasmosis ocular y se incluyeron a 19 pacientes que desarrollaron neovascularización retinal. La frecuencia de NR en pacientes con TO en Argentina fue de 3,16%. El desarrollo de NR fue mayor en pacientes con TO de la provincia de Misiones (5,33%) y fue casi inobservable en pacientes con TO de la provincia de Buenos Aires (0,66%) (p=0,018). Los pacientes con TO de Misiones desarrollaron NR en la zona retinal 2 mientras que la NR observada en pacientes con TO de Santa Fe tuvo una distribución más periférica (p=0,016). La fotocoagulación con láser fue el tratamiento más utilizado para la NR en pacientes con TO. El uso de bevacizumab intravítreo como tratamiento inicial de la NR no logró la completa involución de los vasos retinales.
Conclusiones: La NR en pacientes con TO es una forma infrecuente de presentación clínica en pacientes de la Argentina. Su frecuencia es mayor en las provincias de Misiones y de Santa Fe que en la provincia de Buenos Aires. La fotocoagulación con láser es la terapéutica más utilizada para el tratamiento de la NR en pacientes con TO en Argentina.
Palabras clave: neovascularización retinal, toxoplasmosis ocular, fotocoagulación con láser, bevacizumab, Argentina.
Neovascularização retiniana na toxoplasmose ocular
Resumo
Objetivo: Determinar a frequência de neovascularização retiniana (NR) e as características clínicas oculares de pacientes com toxoplasmose ocular (TO) que desenvolvem esta complicação. Além disso, descrever a forma de tratamento mais utilizada na Argentina nos casos de NR em pacientes com TO.
Materiais e métodos: Foi realizado um estudo clínico retrospectivo onde foram revisados prontuários de pacientes com toxoplasmose de quatro centros de referência em uveítes em 3 regiões do país. Os dados analisados nos prontuários foram acuidade visual no momento da primeira e última consulta, localização e extensão da lesão retiniana e área de neovascularização, tratamento de NR e complicações retinianas.
Resultados: Foram revisados 550 prontuários de pacientes com toxoplasmose ocular e incluídos 19 pacientes que desenvolveram neovascularização retiniana. A frequência de NR em pacientes com TO na Argentina foi de 3,16%. O desenvolvimento de NR foi maior em pacientes com TO da província de Misiones (5,33%) e foi quase inobservável em pacientes com TO da província de Buenos Aires (0,66%) (p=0,018). Pacientes com TO de Misiones desenvolveram NR na zona retiniana 2, enquanto a NR observado em pacientes com TO de Santa Fé teve distribuição mais periférica (p=0,016). A fotocoagulação a laser foi o tratamento mais utilizado para RN em pacientes com TO. O uso de bevacizumabe intravítreo como tratamento inicial do RN não alcançou involução completa dos vasos retinianos.
Conclusões: A NR em pacientes com TO é uma forma incomum de apresentação clínica em pacientes da Argentina. Sua frequência é maior nas províncias de Misiones e Santa Fé do que na província de Buenos Aires. A fotocoagulação a laser é a terapia mais utilizada para o tratamento de RN em pacientes com TO na Argentina.
Palavras-chave: neovascularização retiniana, toxoplasmose ocular, fotocoagulação a laser, bevacizumabe, Argentina.
Introduction
Retinal neovascularization (RN) is defined as the development of small and/or large new vessels creating irregular vascular networks either on the retinal surface or protruding into the vitreous cavity1. RN is a frequent complication of retinal vascular pathologies that produce hypoxia secondary to retinal ischemia such as diabetic retinopathy and central retinal vein occlusion. RN is also found in posterior segment uveitides2. Specific aetiologies of uveitis such as Eales disease and, to a less extent, Behçet disease are frequently associated with RN3. RN was also described in juvenile idiopathic arthritis, sarcoidosis, pars planitis, idiopathic retinal vasculitis, and SLE4. RN in OT was first described by Gilbert in 1980 in a 24-year-old woman with active OT who developed retinal and optic disc neovascularization5. RN presence in a context of active ocular toxoplasmosis has been referred as an atypical OT clinical presentation6. RN was also reported during the inactive period of OT as a source of vitreous hemorrhage7.
Mechanistically, RN is the response of the retinal endothelial cells to the chronic local production of vascular endothelial growth factor (VEGF). VEGF is the main final product of the HIF (hypoxia inducible factor) pathway. This pathway is stimulated by low O2 levels in retinal tissue because of ischemia. In the retina, Muller cells are the main source of VEGF in diabetic retinopathy8. VEGF is also produced during inflammation. Macrophages, more specifically M1 and M2 macrophages promote angiogenesis during chronic stages of inflammation by secreting VEGF-A, PDGF-BB as well as IL-109.
The development of specific monoclonal antibodies against VEGF during the first decade of this century opened new therapeutical opportunities for patients with choroidal and retinal neovascularization. Intraocular injection of anti-vascular growth factor antibodies was shown to be a useful adjuvant in choroidal and retinal neovascularization in uveitis10-11, however no descriptions of treatment with anti-VEGF antibodies for RN in OT patients have been reported.
Worldwide, RN in OT patients is described as atypical or rare. The purpose of this study is to assess its frequency, clinical ocular details and treatment used for RN in OT patients from Argentina.
Material and methods
This is a descriptive retrospective clinical study of RN in OT patients. Three databases from four tertiary referral uveitis centers were reviewed: Consultorio de Uveítis y Glaucoma from Oberá, Misiones (Northeast of Argentina) from September 2012 to December 2020; Oftalmología Global from Rosario, Santa Fe, from January 2001 to March 2021 (Center-Litoral region of Argentina), the Departments of Ophthalmology of the University of Buenos Aires and Austral University from Buenos Aires city and Buenos Aires province, respectively, from January 2011 to February 2019 (Center of Argentina).
This study adhered to the tenets of the Declaration of Helsinki. Clinical records from the uveitis section of each center were reviewed. Patients with OT diagnosis who developed RN during active retinochoroiditis or between reactivation episodes were included in the analysis. Patients with diabetic retinopathy, blood disorders such as hemoglobinopathies or polycythemia vera were excluded.
The four tertiary referral uveitis centers treat every episode of active ocular toxoplasmosis with antiparasitic therapy according to the clinical criteria of the treating physician.
Active OT was defined as (1) the presence of a lesion of retinochoroiditis, associated or not to a previous retinochoroidal scar, with presence of serum antibodies against Toxoplasma gondii or (2) positive polymerase chain reaction findings for toxoplasma deoxyribonucleic acid in the aqueous humor. Retinochoroiditis was defined as the presence of a yellow-white retinal lesion with indistinct borders, accompanied by vitreous inflammatory cells. Retinochoroidal lesions were considered inactive when their borders become discrete and retinochoroidal atrophy and/or pigmentation occurred.
Retinal neovascularization was defined by the presence of small and/or large new vessels creating irregular vascular networks either on the retinal surface or protruding into the vitreous cavity observed by indirect binocular ophthalmoscopy (ETDRS Ophthalmology 1991). Retinal fluorescein angiography or angio-OCT1 was used in order to confirm the diagnosis in specific cases.
Collected data from clinical records included best corrected visual acuity findings at presentation and that corresponding to the last examination, retinal location and extension of the toxoplasmic lesion, retinal location and extension of the retinal neovessels, treatment of the retinal neovascularization (intraocular anti-angiogenic injection, laser photocoagulation, vitrectomy), retinal complications (macular edema, branch retinal vascular occlusion, vitreous hemorrhage, epiretinal membrane, retinal detachment).
Location of retinal lesions, such as OT retinochoroiditis and RN, was defined as described by Holland et al.12, briefly, as in zone 1 when the RT lesion or RN is located between the temporal retinal vessels or around 1 disc diameter to the optic nerve, zone 2 between the retinal temporal vessels or the limits of zone 1 in the nasal retina and the vortex veins, zone 3 between the vortex veins and the ora serrata.
Extension of the OT lesion and of the retinal neovascularization area was determined by comparison with the area of the optic nerve disc.
Consigned retinal complications at the end of the active episode included macular edema, epiretinal membrane, macular hole, macular ischemia, tractional or rhegmatogenous or exudative retinal detachment, branch venous occlusion and branch arterial occlusion.
Term definitions of the ocular inflammatory signs were in agreement with those established by the Standardization of Uveitis Nomenclature Working Group.
Definitions were discussed between all the authors of this study in order to exclude misunderstandings previous to the statistical analysis.
Treatment for ocular toxoplasmosis consisted in either standard oral treatment with pyrimethamine 25 mg/day + sulfadiazine 1-2 g/day or a fixed combination of trimethoprim 160 mg+ sulfamethoxazole 800 mg twice a day plus meprednisone 0,5-1 mg/kg/day and folinic acid 15 mg three times per week. Intravitreal clindamycin (1 mg) was used in patients with retinochoroidal lesions in zone I or patients with active OT during pregnancy.
To compare the RN frequency between centers the X2 test was used. When comparing numerical variables between 2 groups the Mann-Whitney test was used. When comparing 3 groups the non-parametrical Kruskal Wallis test was used. p values were calculated for every analysis and p < 0.05 was considered significant. Statistical analysis was done with SPSS software version 25.0 (SPSS, Inc, Chicago, IL).
Results
After reviewing 550 records of patients with OT, 19 patients who developed RN were included in the present retrospective study (3.16%). The frequency of RN in OT patients depending on the province of the country was as follows: 5.33% in Misiones, 4.0% in Santa Fe and 0.66% in Buenos Aires (Table 1). When comparing RN frequencies in OT patients from Buenos Aires vs of OT patients from Misiones a significative difference was observed (p=0.018). A significative difference was also observed when the RN frequency of OT patients from Buenos Aires was compared vs OT patients from Santa Fe (p=0.048). Development of neovessels was more frequent during active OT in patients from Misiones (62.5%) than patients from Santa Fe (40%) (Figure 1, Table 1). All patients with RN had retinal vasculitis during their last episode of active OT even those who developed RN during the inactive period. Branch vein occlusion was observed in 50% of OT patients that developed RN from Misiones and Santa Fe while branch arterial occlusion was observed in 25% and 10% of OT +RN patients of the above-mentioned provinces respectively.
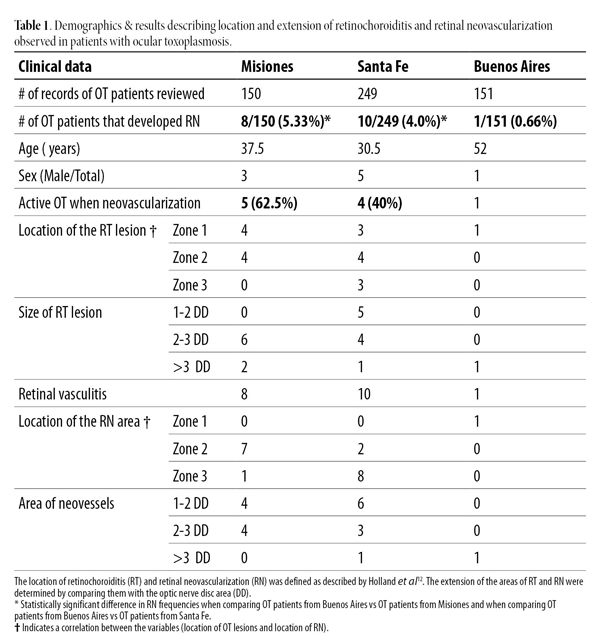
Results on location of the OT lesion in patients who developed RN were as follows: 42.10% in zone 1, 42.10% in zone 2 and 15.8% in zone 3 (Table 1). The distribution of lesions in OT patients from Misiones showed a similar frequency of location in zone 1 and zone 2. OT lesions in patients from Santa Fe distributed homogeneously in the three retinal zones.
The extension of OT lesions in patients who developed RN were equal or bigger than 2DD in 100% of patients from Misiones and in 50% of patients from Santa Fe. RN in OT patients from Misiones located in zone 2 whereas RN in OT patients from Santa Fe located more frequently in the retinal periphery (p=0.016). A mild positive correlation between RN location and OT location was observed (p=0.05, Rho =0.47). There were no differences in the extension area of RN between patients from Misiones and Santa Fe. The patient from Buenos Aires was diagnosed but lost for follow up.
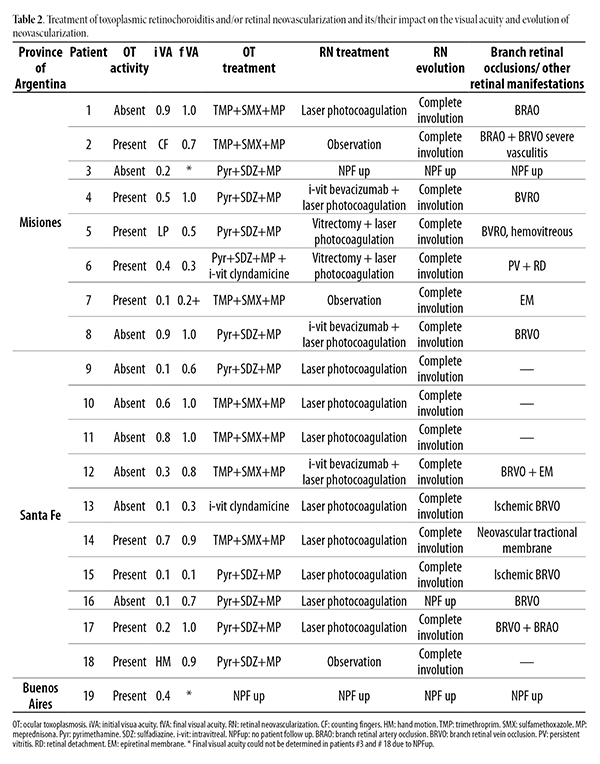
Fifteen patients received specific treatment for RN (Table 2). Nine patients were treated with laser photocoagulation as first line of treatment. Three patients (2 from Misiones and 1 from Santa Fe) were initially treated with 3 doses of intravitreal bevacizumab resulting in incomplete RN regression. The same patients were latter treated with laser photocoagulation (Table 2). All patients that underwent laser photocoagulation had a complete regression of the retinal neovascularization. Two patients (patients # 5 and #6) from Misiones underwent vitrectomy plus intra-surgical laser photocoagulation. Patient #5 due to recurrent vitreous hemorrhage and patient #6 due to retinal detachment. Three patients that developed RN during active retinochoroiditis (patients #2, #7 and #18), and who received systemic treatment for OT (as well as all included patients), were observed for RN regression. Complete involution of RN was obtained in the observed 3 patients without specific RN treatment.
Discussion
Retinal neovascularization is an infrequent complication of ocular toxoplasmosis in Argentinian patients (3.16%). RN frequency is higher (5.33%) in OT patients from Misiones (Northeast of Argentina) than in OT patients from Santa Fe (4.0%, Center of the Litoral region of Argentina) and it is almost undetectable in OT patients from Buenos Aires (0.66%, Center of Argentina) (Table 1). A similar frequency of RN to that observed in OT patients from Misiones was recorded in patients with OT from Brazil when studied by angio-OCT13. The variation in RN frequency depending on the geographical location of Argentinian OT patients is in concordance with previous results describing the frequency of atypical OT in Argentina14. Factors pertaining the parasite15 and/or the host16 could explain the above mentioned observed geographical variations.
RN in OT patients from Misiones located more frequently in zone 2 whereas RN in OT patients from Santa Fe located more frequently in the retinal periphery. The difference in RN location observed when comparing both groups could be explained by differences in the location of RT lesions: while RT lesions in OT patients from Misiones located mainly in zones 1 and 2, RT lesions from patients from Santa Fe were homogenously distributed in all 3 retinal zones.
Even though the number of patients followed throughout treatment were small to obtain significant conclusions (n=17), few observations could be drawn regarding specific RN treatment: first, retinal photocoagulation was the most frequent treatment performed in RN of OT patients; second, three patients resolved RN without specific RN treatment and exclusively with antiparasitic (trimethoprim + sulfamethoxazole or pyrimethamine + sulfadiazine) plus meprednisone treatment, suggesting an important inflammatory component in the development of RN during RRT. Supporting evidence for an inflammatory mechanism of RN during active OT was shown by Knol et al, who reported asymmetrical development of RN in eyes with infectious posterior uveitis of diabetic patients17. Specific cytokines such as Il-1, IL-6, IFN-γ and TNF-α released during retinal inflammation were shown to induce angiogenesis even in the absence of retinal ischemia. Increased expression of IL-1β by microglia and macrophages had been linked to RPE damage and death in age related macular degeneration18-20. Further, IL-1β is the most potent cytokine in inducing VEGFs secretion by retinal pigmentary epithelial cells. The effect is mediated by NF-κB and JAK-STAT pathway, but not by HIF-1α, Sp-1or Sp-3 transcription factors21. The activation of the Il-6 -JAK/STAT-3 signalling axis was shown to mediate neovascularization in an animal model of laser induced CNV22.
Specifically during active OT, De La Torre et al. detected high levels of VEGF in aqueous humor of Colombian patients23. The increase in VEGF in these patients is accompanied by high intraocular levels of IL-6, IL-13 and IL-10 and low levels of IFN-γ, corresponding to a predominant Th-2 type of immune response observed in South American patients24. Further, patients #2 and #6 included in the present study were also studied for IFN-γ and IL-10 levels in aqueous humor during OT activity. They both showed an IFN-γ/IL10 ratio lower than 125, suggesting a predominant Th2/M2 type of immune response during active OT, that may be associated with their development of retinal neovascularization.
Third, the use of bevacizumab as exclusive RN treatment was not enough to induce complete involution of RN in OT patients. Three patients that received 3 doses of intravitreal bevacizumab needed laser photocoagulation to induce complete RN regression. These patients had BRVO as a retinal complication of the OT suggesting that ischemia may have been involved at the origin of the RN. The results, although modest in the number of patients treated, indicates the need for studies testing more powerful anti-VEGF molecules in OT patients. On the other hand, incomplete RN regression after intravitreal bevacizumab treatment can also be explained by the activation of alternative pathways to VEGF during OT associated angiogenesis. One of those pathways is the Tie2 receptor family and their ligands called angiopoietin molecules who are involved in health and stability of endothelial cells. The molecule angiopoietin-2 (Ang-2), an antagonist of the Tie2 receptor, were shown to be elevated during retinal vascular disease and inflammation26. Agonist of Tie2 and inhibitors of Ang-2 are potentials targets of RN during inflammation27 and could potentially be thought as complemental treatments of anti-VEGF therapy in RN during OT. Further studies addressing RN treatment under ischemic conditions during OT are needed to establish the best RN treatment in OT patients.
In conclusion, RN is a rare complication of OT. Its frequency varies according to the geographical location of Argentinian patients. RN frequency was higher in OT Patients from Misiones and was almost unobserved in OT patients from Buenos Aires. Further, OT patients from Misiones developed RN in a more central location than patients Santa Fe. Laser photocoagulation was the most frequent form of RN treatment used in all OT patients.
References
1. Ishibazawa A, Nagaoka T, Yokota H et al. Characteristics of retinal neovascularization in proliferative diabetic retinopathy imaged by optical coherence tomography angiography. Invest Ophthalmol Vis Sci 2016; 57: 6247-6255.
2. Patel AK, Newcomb CW, Systemic Immunosuppressive Therapy for Eye Diseases Research Group et al. Risk of retinal neovascularization in cases of uveitis. Ophthalmology 2016; 123: 646-654.
3. Tugal-Tutkun I, Onal S, Altan-Yaycioglu R et al. Uveitis in Behçet disease: an analysis of 880 patients. Am J Ophthalmol 2004; 138: 373-380.
4. Ebrahimiadib N, Maleki A, Fadakar K et al. Vascular abnormalities in uveitis. Surv Ophthalmol 2021; 66: 653-667.
5. Gilbert HD. Unusual presentation of acute ocular toxoplasmosis. Albrecht von Graefes Arch Klin Exp OphthaImol 1980; 215: 53-58.
6. Smith JR, Cunningham ET Jr. Atypical presentations of ocular toxoplasmosis. Curr Opin Ophthalmol 2002; 13: 387-392.
7. Gaynon MW, Boldrey EE, Strahlman ER, Fine SL. Retinal neovascularization and ocular toxoplasmosis. Am J Ophthalmol 1984; 98: 585-589.
8. Rodrigues M, Xin X, Jee K et al. VEGF secreted by hypoxic Müller cells induces MMP-2 expression and activity in endothelial cells to promote retinal neovascularization in proliferative diabetic retinopathy. Diabetes 2013; 62: 3863-3873.
9. Anders CB, Lawton TMW, Smith HL et al. Use of integrated metabolomics, transcriptomics, and signal protein profile to characterize the effector function and associated metabotype of polarized macrophage phenotypes. J Leukoc Biol 2022; 111: 667-693.
10. Mansour AM, Mackensen F, Arevalo JF et al. Intravitreal bevacizumab in inflammatory ocular neovascularization. Am J Ophthalmol 2008; 146: 410-416.
11. Singh SR, Fung AT, Fraser-Bell S et al. One-year outcomes of anti-vascular endothelial growth factor therapy in peripapillary choroidal neovascularisation. Br J Ophthalmol 2020; 104: 678-683.
12. Holland GN, Buhles WC Jr., Mastre B, Kaplan HJ. A controlled retrospective study of ganciclovir treatment for cytomegalovirus retinopathy: use of a standardized system for the assessment of disease outcome. UCLA CMV Retinopathy Study Group. Arch Ophthalmol 1989; 107: 1759-1766.
13. De Oliveira Dias JR, Campelo C, Novais EA et al. New findings useful for clinical practice using swept-source optical coherence tomography angiography in the follow-up of active ocular toxoplasmosis. Int J Retin Vitreous 2020; 6: 30.
14. Schlaen A, Colombero D, Ormaechea S et al. Regional differences in the clinical manifestation of ocular toxoplasmosis between the Center and Northeast of Argentina. Ocul Immunol Inflamm 2019; 27: 722-730.
15. Bernstein M, Pardini L, Moré G et al. Population structure of Toxoplasma gondii in Argentina. Infect Genet Evol 2018; 65: 72-79.
16. Rudzinski M, Khoury M, Couto C, Ajzenberg D. Reactivation of ocular toxoplasmosis in non-Hispanic persons, Misiones province, Argentina. Emerg Infect Dis 2016; 22: 912-913.
17. Knol JA, van Kooij B, de Valk HW, Rothova A. Rapid progression of diabetic retinopathy in eyes with posterior uveitis. Am J Ophthalmol 2006; 141: 409-412.
18. Eandi CM, Messance HC, Augustin S et al. Subretinal mononuclear phagocytes induce cone segment loss via IL-1β. Elife 2016; 5: e16490.
19. Natoli R, Fernando N, Madigan M et al. Microglia-derived IL-1β promotes chemokine expression by Müller cells and RPE in focal retinal degeneration. Mol Neurodegener 2017; 12: 31.
20. Wooff Y, Man SM, Aggio-Bruce R et al. IL-1 Family members mediate cell death, inflammation and angiogenesis in retinal degenerative diseases. Front Immunol 2019; 10: 1618.
21. Nagineni CN, Kommineni VK, William A et al. Regulation of VEGF expression in human retinal cells by cytokines: implications for the role of inflammation of age-related macular degeneration. J Cell Physiol 2012; 227: 116-126.
22. Izumi-Nagai K, Nagai N, Ozawa Y et al. Interleukin-6 receptor-mediated activation of signal transducer and activator of transcription-3 (STAT3) promotes choroidal neovascularization. Am J Pathol 2007; 170: 2149-2158.
23. De-la-Torre A, Pfaff AW, Grigg ME et al. Ocular cytokinome is linked to clinical characteristics in ocular toxoplasmosis. Cytokine 2014; 68: 23-31.
24. De-la-Torre A, Sauer A, Pfaff AW et al. Severe South American ocular toxoplasmosis is associated with decreased Ifn-γ/Il-17a and increased Il-6/Il-13 intraocular levels. PLoS Negl Trop Dis 2013; 7: e2541.
25. Rudzinski M, Argüelles C, Couto C et al. Immune mediators against Toxoplasma gondii during reactivation of toxoplasmic retinochoroiditis. Ocul Immunol Inflamm 2019; 27: 949-957.
26. Scholz A, Plate KH, Reiss Y. Angiopoietin-2: a multifaceted cytokine that functions in both angiogenesis and inflammation. Ann N Y Acad Sci 2015; 1347: 45-51.
27. Nguyen QD, Heier JS, Do DV et al. The Tie2 signaling pathway in retinal vascular diseases: a novel therapeutic target in the eye. Int J Retina Vitreous 2020; 6: 48.